This World AIDS Day the world is facing perhaps the most complex political and epidemiologic environment in the history of the global AIDS pandemic. To tackle this environment we need an equally sophisticated response that builds new evidence for what’s really working at a macro level, refuses to accept the current funding realities, and mobilizes human rights frameworks in powerful new ways to advance the fight against HIV.
The good news of the moment is that the new UNAIDS report shows that the pace of HIV treatment scale up has increased for the third year in a row—with a net of 2.7 million new people added to treatment and a total of 20.9 million accessing treatment. This reflects shifts in HIV policies across the world toward treatment for all without requiring people living with HIV to wait to reach a certain CD4 level (damage to the immune system) before starting. The more troubling news is that HIV funding is deeply in peril. For the second year in a row the Kaiser Family Foundation found that international aid funding to fight HIV declined—by US$511 million from US$7.5 billion to US$7 billion. While national governments in countries with high HIV burden are increasing their funding to fight AIDS, the pull back in donor funds threatens scale up across the board.
This is an especially perilous moment in the history of the epidemic because things are going right on many fronts—but progress could not be more fragile and the relative success in some areas means that reaching the rest gets harder not easier. For example in many of the countries with the highest rates of HIV in the world a significant portion of people living with HIV know their status. On average in East and Southern Africa UNAIDS reports that 76% of people know their status and in South Africa the estimate is 86%. While this is a huge success, these countries continue to have large numbers of new HIV transmissions. This is in part because many who know their status are not on effective HIV treatment to halt transmission and HIV-negative people have limited access to proven HIV prevention technologies. But it is also likely that many of those who do not know their status—the 25% who are hardest to reach—are among those having sex and experiencing HIV transmission. Younger people in their 20s, for example, are among the most sexually active populations yet have far lower knowledge of their status while key populations such as men who have sex with men are less likely to know their status and successfully suppress the virus than their peers in many countries. So we have to start thinking differently and acting on the epidemic we face in 2018 not the one we faced a decade ago.

Researchers in KwaZulu-Natal South Africa
We need, in 2018, to be far more serious and precise about the impact of international efforts to fight HIV and the intersection of aid dollars and the national health system. Here at Georgetown’s O’Neill Institute we recently launched a new project with South African researchers to look at exactly how donor funded efforts are augmenting the national response at front-line facilities. We hope to start understanding a bit better how policies set at the highest levels, specifically regarding which funding source will support which services, play out by the time those policies trickle down to what people in health facilities experience.If we are serious about achieving global goals on HIV there is no alternative to increasing the efficacy and impact of these funds. Ours is a small contribution to the broader agenda that PEPFAR, the Global Fund, the World Bank, and other HIV financing agencies need to address head on—in an era of still growing needs, how can international funds build synergies in practice, not just in theory, with clear and identifiable benefit for communities affected by HIV?
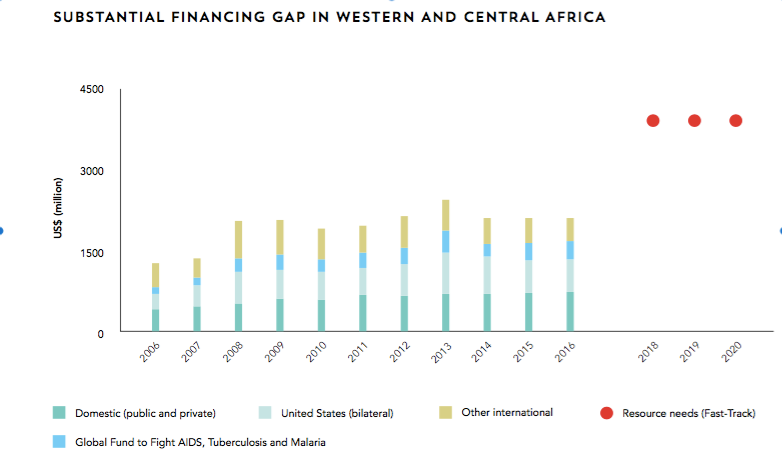
West & Central Africa Funding Gap
Even if we succeed in increasing the efficacy of the funding we have there is no way out of the reality that more funds are needed. Recent data have shown, for example, that in the places where funding has been sufficient we have achieved key milestones against HIV. Where it’s not, we are failing. East and Southern Africa, for example, has seen ambitious levels of funding including from international sources like PEPFAR and Global Fund that are driving powerful results—like the recent evidence from the PHIA studies showing remarkable progress toward “epidemic control” in key countries. These striking results mean that HIV could move from a crisis to a manageable epidemic in these countries, but only if resources are sufficient to take scale up through to success. This it stands in stark contrast to West and Central Africa where funding has lagged far behind and, as a result, the region has just 35% of PLHIV on treatment and just 25% of all PLHIV achieving viral suppression.
We have to be serious about where the challenges are. A spate of good news in select East and Southern African countries is showing what’s possible. But over-emphasis on some leading countries—where it must be noted far more work is still required to turn possibility into reality—could blind us to the broader needs. The recent PEFPAR strategy is just one example—setting out what are notably ambitious goals for 13 key countries. But with neither PEPFAR nor Global Fund sufficiently financed for the task at hand, neither has a strategy to address the broader context in which the country facing the largest number of new HIV infections, South Africa (not one of the 13), is not on track to reach “epidemic control” as originally planned, countries in the region like Angola and Mozambique are further from success, and epidemics in West Africa led by those in Nigeria and Cameroon are not being met with anywhere near the level of effective response as in the South. Diagnosing the problem correctly has to be part of the solution in a pandemic that follows trade routes not national borders.
Finally, we need to start treating human rights as a truly integral part of the strategy to attack the HIV pandemic. My research has shown that countries that protect a constitutional right to health perform better on key health indicators—and HIV is a key part of that story. Where rights are well enshrined and, most importantly, where rights-supporting organizations like Section 27 in South Africa, Kelin in Kenya, CEHURD in Uganda, and many more are well funded, there is a real opportunity. In these contexts, policy actors seeking to advance access and equity are better able to break into closed bureaucratic policy cycles and force issues ranging from how budgets are spent to which drugs are available to whom into the open. It holds the potential to make HIV and health policy better than it would otherwise be at tackling real life challenges. The most recent UNAIDS report focused in on the Right to Health and with good reason. In 2018, Human Rights have to move beyond first generation rights and the important role they have played in protecting people living with HIV from discrimination and avarice and take the rights of access to scale—in the court rooms, but most importantly outside in all the venues where policy is made.
All of this comes at a time of rising global populism and weakened international institutions. Yet time and time again the global AIDS response has overcome seemingly intractable contexts—breaking the power of multinational pharmaceutical companies to set high prices and expanding financing for scale up through the global financial crisis are just two examples. The coming years, though, are likely to dictate the course of the epidemic—we can miss this opportunity because it is too complex for easy slogans or we can be real about the challenge and use all the tools of 2018 to halt HIV.
—
Matthew Kavanagh, PhD is visiting professor at Georgetown University and director of the Global Health Policy and Governance Initiative at the O’Neill Institute.


