In early November, a Center for Innovation in Global Health (CIGH) team visited Malawi to support ongoing implementation of the Blantyre Prevention Strategy (BPS), a Bill and Melinda Gates Foundation grant to CIGH. BPS – an innovative, five-year, systems-focused approach to HIV prevention co-developed by Government of Malawi and CIGH experts in support of government efforts towards long‑term HIV epidemic control – launched in May 2020 during the height of the COVID-19 lockdowns. Despite all the challenges to virtual collaboration, including three COVID waves in Malawi, BPS has thrived under government leadership and with the steady technical support from CIGH and an outstanding consortium of civil society and other partners.
On this World AIDS Day, UNAIDS has called for transformative measures to be taken if we are to get back on track to ending AIDS by 2030. After dozens of meetings in Malawi over the past few weeks, our confidence has only grown that the innovative BPS global health model is one such transformative measure — and is on track to change the way future HIV prevention programs are designed and implemented.
Figure 1. New Approach to Global Health Programs.
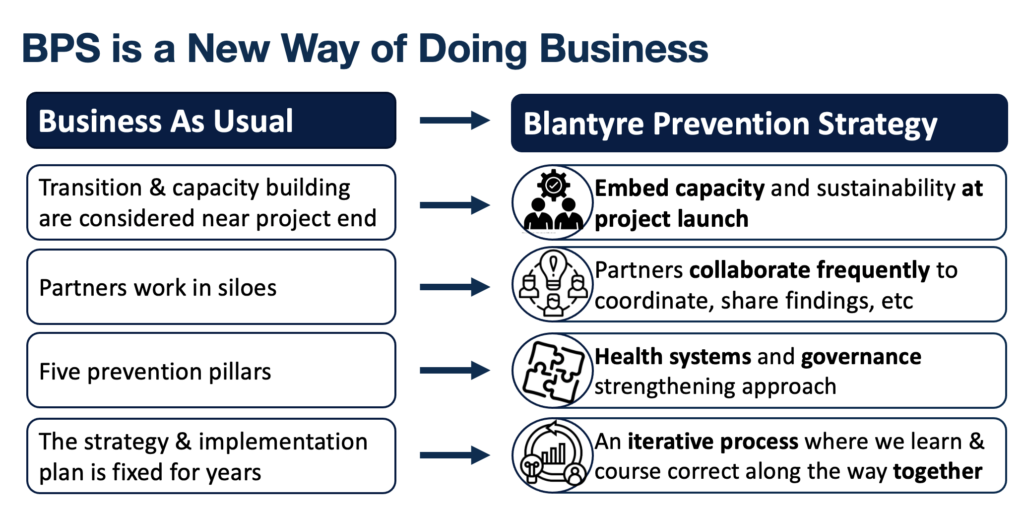
BPS was designed from the start to promote a new way of doing business in four principal ways (figure 1). First, capacity building and sustainability planning have been built into all aspects of implementation. Three governance structures under the leadership of government monitor and guide implementation. BPS expert partners work together with the government at district, city, and national levels to build and institutionalize core prevention cascade capabilities and health systems capacities (figure 2) at district level for effective HIV prevention program design and management. The work is coordinated locally by an experienced program coordinator hired through the National AIDS Commission and seconded to Blantyre District and City.
We saw the effectiveness of this approach during our visit, including during a working group meeting for the pilot bringing HIV into the Blantyre District Health Office’s (DHO) Integrated Disease Surveillance and Response (IDSR). In this case, the DHO leads on pilot implementation, but the supporting working group includes CIGH and BPS‑funded partners providing technical support to the DHO on indicator development, data collection, detection, investigation and HIV prevention response to HIV risk events, community engagement, training for the health surveillance assistants, and project management. The partners are not implementing their work separately from the District Health Management Team (DHMT). Rather, everything is done in collaboration with and under the direct supervision of the DHO and in coordination with the national IDSR program and the Public Health Institute of Malawi (PHIM).
Second, BPS-funded partners do not work in silos. They collaborate with each other through regularly scheduled weekly, monthly, and quarterly meetings, and through facilitated interactions with critical partners such as those funded for HIV prevention service delivery and technical support in Blantyre by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). This collaboration has been powerful and identified new ways for partners to leverage each other’s data and programs. For example, a three-day workshop focused on use of new data collected through three studies, including data on public and private HIV prevention service delivery and a network mapping of community-based organizations (CBOs) in Blantyre. Participants, including government, BPS-funded partners, PEPFAR implementing partners, and local civil society and community groups, worked in small groups to review and identify ways to use the data effectively to support HIV prevention and prioritization of resources by the district. In addition to making new connections with each other, partners identified issues and opportunities for improved programming, such as engaging with CBOs working in isolation and using the data to target mobile services.
Figure 2. Key BPS Work Streams Aligned to the HIV Prevention Cascade
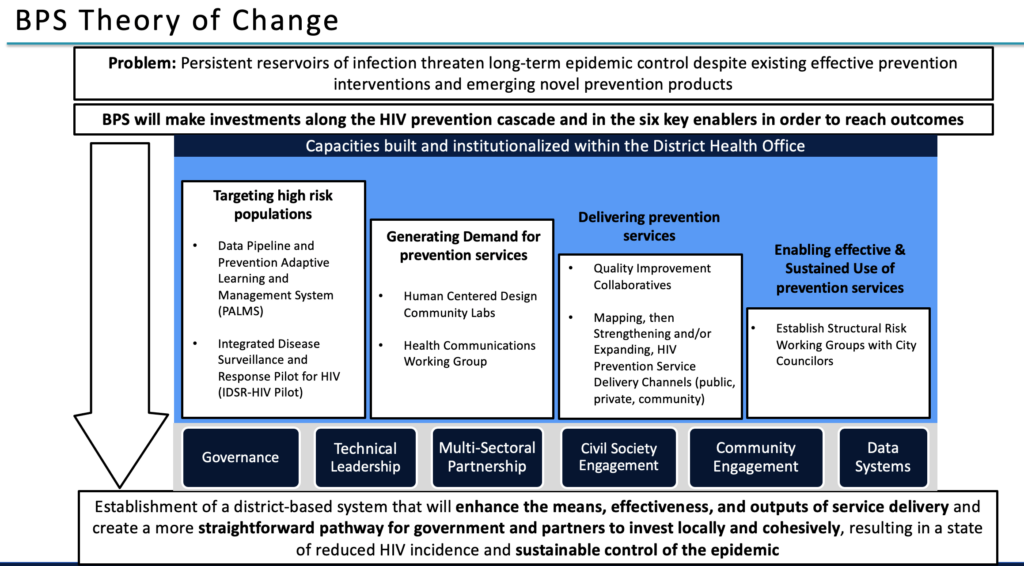
Third, BPS is a health systems innovation-focused project aimed at strengthening and improving the impact of existing investments and demonstrating effective pathways for further local investments for government, PEPFAR, and Global Fund. BPS invests directly in improving Blantyre City and District’s abilities to detect and target disease risks, generate demand for prevention services based on risks, effectively deliver prevention products and interventions, and enable effective and sustained use of prevention products by the citizens of Blantyre. BPS work streams (figure 2) align with these prevention cascade elements and mutually reinforce each other (e.g., higher intervention quality leads to improved community demand). This approach is already paying dividends through PrEPUp!, the BPS quality improvement (QI) collaborative focused on pre-exposure prophylaxis (PrEP) run through the DHO quality unit and coordinated with the sites and partners supporting PrEP services in each facility. This partnership has identified ways that PrEPUp! can address delivery challenges.
National and local governance is key to the BPS approach. During our visit, we met with the Ministry of Health’s Secretary for Health (SH) who chairs the BPS Steering Committee, the Ministry’s Director of the Department of HIV/AIDS and Viral Hepatitis, and the NAC acting Chief Executive Officer. Their leadership and active engagement is not limited to periodic governance meetings. Their depth of understanding about BPS and commitment to its objectives has been essential to progress already made. The SH reiterated his commitment to using BPS’s learning to inform evidence-based policies given the centrality of BPS to the country’s efforts to control HIV.
Fourth, the cornerstone of the BPS approach is its learning agenda. The platform was developed to promote dynamic sharing of learning that rapidly identifies opportunities for course corrections and program iterations to enhance outcomes and impact. Partners are utilizing real-time learnings from parallel work streams to inform and adapt activities for maximum coordination and project impact. While in Malawi, the NAC Director of Programs convened the BPS Consortium to discuss work stream progress as well as look holistically at learning about PrEP demand generation and delivery. From the data pipeline and public, private, and community service delivery mapping, the group learned about gaps in service coverage that provide opportunities for improved targeting. From the community labs, we learned about solutions identified to improve demand generation for oral PrEP among adolescent girls and young women and female sex workers. PrEPUp! demonstrated the process maps developed by the 21 public and private facilities to improve screening for, referrals, and delivery of PrEP.
World AIDS Day marks an annual opportunity to spotlight the HIV pandemic and the continuing toll on 38 million people living with HIV globally, including nearly 1 million in Malawi. Key to achieving the global goals of ending the HIV pandemic as a public health threat by 2030 is dramatically reducing new infections. UNAIDS has also called for a paradigm shift in more locally driven HIV responses to achieve those goals. BPS’s district-led approach — embedded within local systems and capabilities — provides one such model that aims to systematically enhance the deployment and uptake of HIV prevention interventions and achieve sustained control of the HIV epidemic. Spending two weeks working together in person in Malawi convinced us that we are well on our way to meeting these objectives and identifying important lessons that can assist other districts and localities in the region improve HIV prevention.

