Pre-exposure prophylaxis, or PrEP, is a medication that people at risk for HIV take to prevent HIV acquisition. When taken as prescribed, it is highly effective for preventing HIV acquisition. Despite its efficacy, PrEP uptake has been relatively low in the United States, in part because the cost of the medication can pose a financial challenge for people, even if they have insurance. But beginning on January 1, 2021, most health plans in the United States must cover the full cost of PrEP, thanks to the enforceable recommendation of the U.S. Preventive Services Task Force (USPSTF). The USPSTF is a federally appointed independent panel of physicians and other experts that reviews the scientific literature and makes evidence-based recommendations for the use of clinical preventive services such as screenings, counseling services, and preventive medications. In June 2019, the USPSTF issued a final “Grade A” recommendation for PrEP, meaning that there is strong evidence supporting the use of PrEP by persons at high risk for HIV. This recommendation requires that PrEP be covered by most health plans without cost sharing (i.e., no copay, coinsurance, or deductible). Under the Affordable Care Act (ACA), nearly all private health plans and all Medicaid-expansion programs must cover services that receive a Grade A or Grade B rating from the USPSTF without cost sharing in the plan year that begins one year after the date of the recommendation.
Substantial evidence showing that PrEP significantly decreases the risk of HIV acquisition has reinforced the view that ensuring stable and affordable access to PrEP services is crucial to the success of the Ending the HIV Epidemic Initiative (EHE) in the United States. Unfortunately, HIV+Hepatitis Policy Institute and other organizations found that many health plans have not yet complied with the USPSTF’s legal requirement, despite having months to prepare. According to CDC data, less than 10% of the 1.1 million people who could benefit from PrEP are taking it, in part because out-of-pocket annual costs for the medication can exceed $1,000. Any delay in compliance with the USPSTF’s rule will continue to restrict access to people who need PrEP but cannot afford it. Other significant barriers to PrEP uptake include lack of proper education. People often don’t understand their own HIV risk, or what PrEP is. Many people also experience stigma from health care providers and a lack of open and non-judgmental spaces to discuss their sexual behaviors. To achieve the EHE’s goal of reducing the number of new HIV transmissions by 90% by 2030, the number of people from the communities with the highest HIV prevalence who are using PrEP must increase.
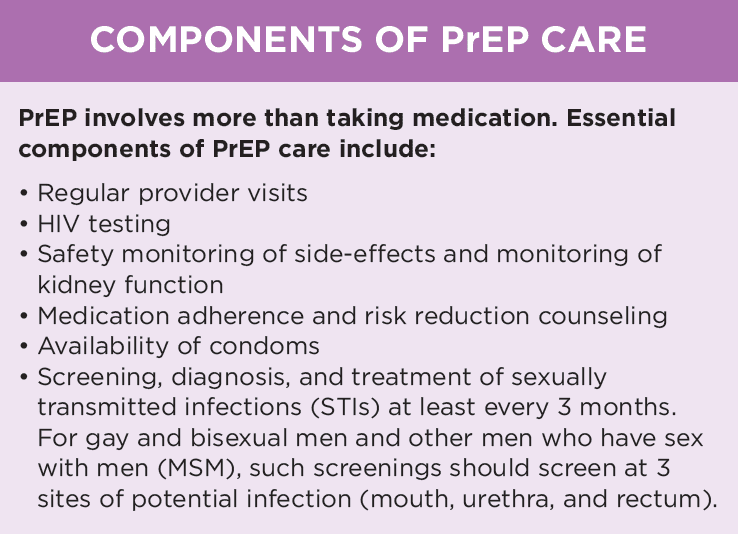
The USPSTF’s PrEP recommendation is a great step forward and should be celebrated, but more work is needed to keep moving forward. First and foremost, all health plans must comply with the legal requirement to offer PrEP without cost sharing. In addition, effective PrEP services involve more than the medication alone. For PrEP to work as it did in the studies that contributed to the USPSTF’s recommendation, health plans must cover ancillary services. These services include routine provider visits and specimen collections, medication adherence and risk reduction counseling sessions, access to condoms, regular laboratory monitoring, HIV testing, and screening and treatment for sexually transmitted infections. Such services are necessary to support effective and ongoing PrEP use to prevent users from acquiring HIV.
Some states, like Colorado’s Department of Regulatory Agencies, have released statewide recommendations fully supporting the coverage of these ancillary services. The Center for Consumer Information and Insurance Oversight (CCIIO) should issue additional federal guidance, specific to the items and services that are integral to providing PrEP (which is consistent with past CCIIO implementation practices for other USPSTF recommendations). This guidance will establish more uniform standards for health departments and providers. Further, health plans should not require prior authorization once a provider has prescribed PrEP services. Health departments should also track PrEP uptake in their jurisdictions and publish public dashboards to promote broader and more equitable PrEP use. Health care providers and community members also have critical roles in monitoring health plans and supporting models of PrEP delivery that increase access to PrEP.
To ensure that the delivery of PrEP services is an effective intervention for achieving population-level reductions in new HIV cases, more attention is needed to support effective implementation. In a prior release, Quick Take: The USPSTF Recommendation, we explore several of these implementation actions. The USPSTF PrEP recommendation can be a major contributor to fewer HIV transmissions—if it is implemented appropriately.
Sean Bland, J.D., is a senior associate of the Infectious Diseases Initiative at the O’Neill Institute for National and Global Health Law.
Landon Myers, J.D., is a law fellow at the O’Neill Institute for National and Global Health Law.