Invisibility is not an accident in global health — it is a design flaw.
Rodah Bhulabhula’s story is one example. She is a young woman from rural Zimbabwe, who grew up without access to sunscreen or preventive care. As a result, she suffered from painful sun blisters and sores, which led to bullying at school and eventually to her dropping out. She turned to subsistence farming, a job requiring her to spend entire days toiling in the hot sun, developing painful sunburns. Rodah had no way out. Avoiding the sun meant losing her only source of income. Her wages, below $100 a month, allowed for sustenance, but were not enough to cover the sunscreen she needed, which costs between $15 and $20 per bottle. Rodah developed skin cancer and had her left eye removed due to a cancerous tumor, forcing her to cease her farming activities altogether.
The hope is that Rodah’s story will be the last in the line of unnecessary suffering for people with albinism. Invisible on global health agendas for far too long, albinism-related health issues have been underfunded and underprioritized.
In September 2025, the World Health Organization added sunscreen to its list of essential medicines, a potential game changer for an estimated 170,000 to 300,000 people living with albinism in sub-Saharan Africa.
People with albinism are 1,000 times more likely to develop skin cancer, and suffer disproportionately, as well as experiencing face stigma, marginalization, poverty, and a shortened life expectancy. Until recently, sunscreen, long classified as a cosmetic product, thus a luxury good subject to import tax, remained out of the economic reach of those who needed it the most.
Skin cancer is preventable, where the use of a hat or applying sun screen are simple interventions that could save lives. Still, 98% of people in LMICs with albinism will not live to see their fortieth birthday. While no disaggregated data exists globally to indicate how many persons with albinism develop skin cancer, civil society data from several countries show high rates of skin lesions and preventable deaths among persons with albinism.
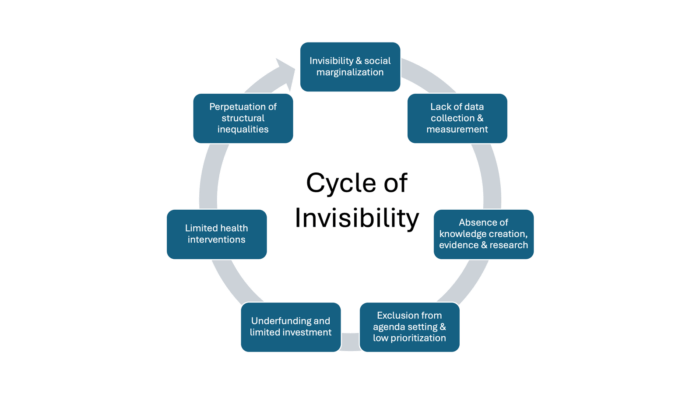
Conditions, such as albinism, that are hard to measure, slow to solve, impact a relative few, or require a whole-system-non-vertical approach are systematically deprioritized. Structural inequalities — particularly economic and epistemic — shape which health outcomes are measured, whose voices are heard, and whose suffering is acknowledged, and who is measured. The vicious cycle of invisibility emerges, functioning as both a cause and an effect. The groups that often lack the institutional power to influence knowledge creation are then less likely to be measured, studied, or prioritized. What cannot be measured cannot be helped. Data is essential to ensure that decision-makers put health conditions on agendas. Albinism — a rare genetic condition that disproportionately impacts a marginalized community — exemplifies this dynamic, suffering limited attention within global health frameworks. Disrupting this cycle depends on addressing the systemic factors that marginalize certain conditions.
In the case of albinism, this cycle has begun to break through the efforts of multiple actors. The creation of the mandate of the United Nations Independent Expert on the Rights of Persons with Albinism in 2015, led by a woman with albinism, helped to bring global attention to albinism issues. Secondly, civil society and advocacy groups engaged in targeted advocacy efforts, highlighting skin cancer as a major health issue in the albinism community.
At the local level, civil society organizations partnered with research institutes to document the health experiences of persons with albinism, such as the 2025 report on the experiences of persons with albinism affected by skin cancer in Zimbabwe. These stories were highlighted on the COP 30 global stage by Gwen Mushonga, a Zimbabwean female activist. At a systemic level, advocates submitted scientific, human rights-based, and medical evidence to the WHO lobbying for the inclusion of sunscreen lotion on the Essential Medicine List. Finally, an amicus brief on the right to health filed before the African Court of Human and Peoples Rights resulted in a judgment affirming governments’ obligations to provide universal access to sunscreen lotion to protect the right to health, thereby generating a strong legal grounding for ongoing actions.
The addition of sunscreen to the WHO Essential Medicines List follows a historic African Court ruling in February, which affirmed that sunscreen, wide hats, and sunglasses are essential, not luxury items, for persons with albinism — comparable to access to safe drinking water.
Breaking this cycle of invisibility of health diseases requires:
- A shift in power for priority setting
- Decolonization in knowledge production to ensure that the invisible are included in how health systems count, collect, and define global health problems
- Expansion of disaggregated data collection to highlight overlooked issues deemed as urgent by affected communities
- Refocusing on the central tenet of the right to health, regardless of the disease or location
The UN has identified the global dearth of data on the number of persons with albinism in national datasets as problematic, urging countries to reform their collection processes. The lack of knowledge about albinism among health care providers results in a lack of quality health care services to promote the highest attainable standard of health.
Beyond Survival, Access to Holistic Healing is an Equity Issue
For people with albinism, like Rodah, if pre-cancerous lesions are not addressed early and treated, the lesions develop into deep wounds that require surgical excision to prevent skin cancer from spreading. The surgery is essential for survival, and yet often results in deep scarring. While those scars represent a lifeline, they can also lead to mental anguish and deepen the social stigma because of the resulting deformity. Reconstructive surgery is all too often misclassified as a luxury in global health, and yet it is essential for mental health, dignity, and improved quality of life.
Global surgery, which can be both life-saving and life-changing, provides an interesting parallel journey with albinism in that it is widely absent from donor agendas. Dr. Paul Farmer famously called global surgery the “neglected stepchild of global health,” which was before the 2015 landmark publication of the Lancet Commission on Global Surgery. 2015 was a watershed year for both global surgery and albinism, with these issues getting into the lexicon of multilateral agencies. And for people with albinism, they suffered a double burden of needing attention to both interconnected health interventions.
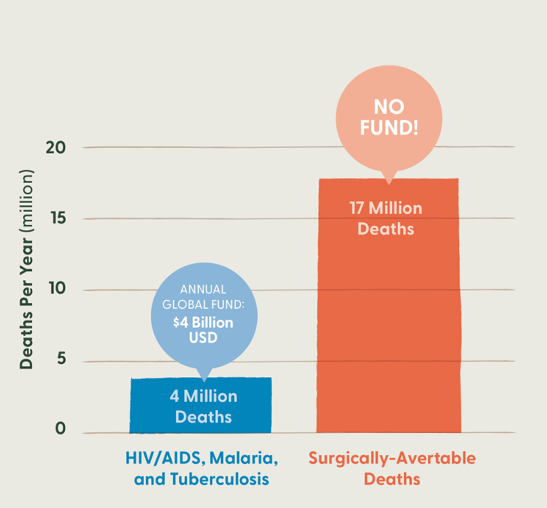
Global surgery impacts the vast majority of the global population, with 5 billion people lacking access to safe, affordable, and timely surgery. Not only is it lifesaving, but global surgery also has the ability to completely change a person’s quality of life, restoring function to return to work or school. Surgically avertable mortality makes up 17 million deaths annually (primarily from traumatic injuries and obstetric emergencies), three times that of HIV, malaria, and tuberculosis combined. While reconstructive surgical services can mistakenly be labeled as “non-essential,” they can decrease disability and vastly increase quality of life. Similarly, access to sunscreen lotion as an essential medicine can ensure that children with albinism can safely go to school and play, adults can work, and also live fuller and more productive lives, protecting their skin from harmful UV radiation. Labeling sunscreen for people with albinism and reconstructive surgery as “luxuries” exposes deep inequities in the prioritization of global health interventions: care that prevents suffering, restores dignity, and function are vital, and should not require proof of worthiness.
The Data Is Clear, Now the Funding Must Follow
For albinism and global surgery data have proven essential in proving the scale and impact of the problem. Yet, both health interventions have a long way to go, as the funding has yet to catch up to meet the scale of the need.
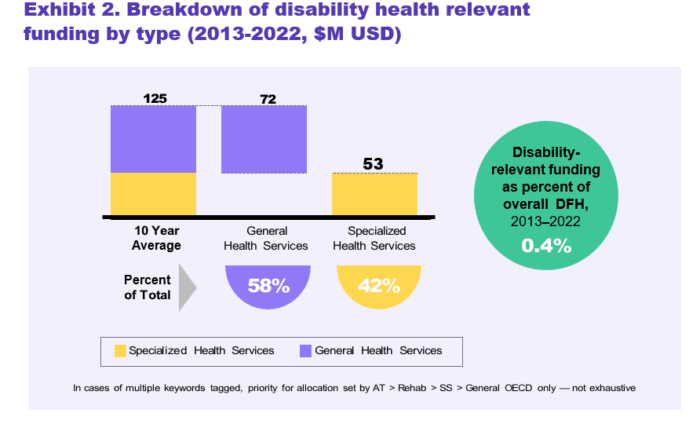
Studies have found that in order to improve the care of patients with albinism, surgeons need educational seminars on skin cancer, surgical techniques for skin cancer removal, and knowledge and skills on reconstructive surgery. Yet, funding for disability-inclusive healthcare continues to be deprioritized. In 2025, reportedly only 0.4% of all development financing for health is, on average, disability-relevant.
Consequently, persons with disabilities are more likely to experience barriers to care, including the lack of care when they need it due to the non-existence of services or cost-related barriers. Data has helped to get these public health issues on the map, the next challenge will be reducing the stark mismatch between disease burdens and funding. More work must be done to reframe both preventive treatment for people with albinism and surgery to prove that they are, in fact, essential services that save lives, as well as improve the quality of those lives, which merit desperately needed investment.
Making the Invisible Visible
Rodah’s story is not just about one woman with albinism in Zimbabwe. It is a mirror held up to the global health system itself: a system that treats sunscreen as “luxury,” causing Rodah to lose her left eye when prevention was just a sunscreen bottle away. For millions, accessing these health interventions means survival, dignity, and the possibility of a full life. The same dynamics that left Rodah unprotected are what keep countless other conditions invisible — considered too niche, too expensive, or too complex to address on donor agendas.
Equity demands that those in the shadows be made visible through investment in knowledge generation, prioritization, funding, and intervention on their unique health issues. The recent advocacy successes for albinism show us a pathway in which the acknowledgment of interventions, such as adding sunscreen to an essential medicines list, can reverberate around the world: reducing unnecessary suffering and allowing broader access to critical health interventions, regardless of the health condition in question. Health should never be a luxury only afforded to those with diseases deemed “worthy” of care.
The question is no longer whether policymakers can act: the solutions, such as sunscreen, already exist. The question is whether we are willing to recognize the invisible, and to count what has long been ignored.
DISCLAIMER: The views and opinions expressed in this piece are those of the authors and do not reflect the views of the O’Neill Institute.

