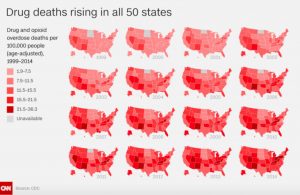
Two weeks ago, CNN released a great informative guide to American on drugs. After reaching out to every state for the latest statistics on drug deaths, they found that drug deaths continue to rise rapidly in many states, especially deaths due to overdoses. Drugs are now the leading cause of accidental death in this country, having overtaken both car accidents and shootings (even more concerning, considering gun deaths have slowly been on the rise in the last two decades). 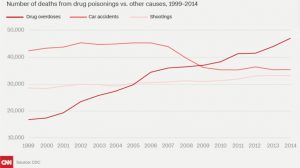
Initially one might think that these overdoses are due primarily to the use of illegal drugs like heroin, meth and crack cocaine– drugs usually perceived as more dangerous and addictive. However, the reality is far more concerning; between 1999 and 2014, more than 165,000 Americans died from prescription-opioid overdoses and in 2014, out of the 28,647 opioid related deaths (61% of all US drug overdose deaths), only 10,574 were related to heroin. This means almost 40% of all drug overdose deaths occur due to legal substances.
This is not to say that illegal drug deaths are not also an increasing problem; heroin related deaths have also been on the rise, increasing 439% from 1999 to 2014, and tripling in the last five years. According to CDC, data from 2014 reflects “two distinct but interrelated trends,” a longterm increase in overdose deaths due to prescription opioids and a surge in illicit opioid overdose deaths, mostly related to heroin. So what explains this sudden rise?
The rise of opioids in America
Before looking at the overdose problem, we have to understand exactly what opioids are and what they do. Opioid painkillers stimulate receptors in the brain and elsewhere to reduce the perception of pain. They help lessen anxiety and depression—two common side effects of intense pain. Some people also experience a feeling of euphoria, since these drugs affect the regions of the brain involved in reward. Some opioids, such as morphine, come from the poppy plant; others, such as oxycodone, are semi-synthetic or synthetic. Regardless of how they are made, they all have the propensity to be highly addictive: even brief use can be followed by withdrawal symptoms.
As a result, for most of the 20th century opioids were usually reserved for acute pain, after a serious accident or surgery, or as palliative care for patients with illnesses such as cancer or AIDS. But starting in the 1980s, a series of papers by American researchers claimed that opioids could be used safely for longer periods. Although the evidence to support this was weak, strong marketing efforts by drug companies led to American doctors prescribing opioids with abandon for chronic, non-terminal pain. Drugs that were once reserved to treat the most extreme pain and terminal illnesses became the solution for moderate pain relief.
While in most countries, the use of opioids is still limited to acute hospitalization and trauma, the U.S. has taken a radically different path. Americans are now taking six times more prescription opioids per person than 20 years ago. As described by the U.S. Surgeon General Vivek Murthy, every adult in America can have “a bottle of pills and then some.” Sadly, his description is hardly an exaggeration; in 2015, there were 227 million prescriptions written for opioids, which is almost enough to provide every American adult with a bottle of opioid pills.
There are states where the situation is even worse. Alabama leads the list of eight states with more opioid prescriptions than residents, with a rate of 1.2 prescriptions per resident! Some of these southern states on the list write almost three times as many prescriptions as those in the lowest prescribing state, Hawaii. Yet there is no evidence to show that there are any underlying health differences in these state’s populations to explain these differences. The same occurs at the national level: while sales of prescription opioids in the U.S. have nearly quadrupled in the last 25 years, there hasn’t been an overall change in the amount of pain Americans report.
With only 5% of the world’s population, Americans now consume the vast majority of opioids (almost 80%), including 99% of the world’s hydrocodone, 80% of the oxycodone and 55% of the morphine. Opioids have become such a common place in the U.S. that the 38% of the population now using prescription painkillers, outnumbers those using tobacco (31%).
The problem with overprescribing
The rise in opioid overdose deaths has occurred alongside this increase in prescriptions. In states like Utah, for example, a direct correlation between the rise in prescriptions and opioid overdoses exists. In 2014, 32% of Utah adults aged 18 years and older had been prescribed an opioid as pain medication, according to the Utah Department of Health Behavioral Risk Factor Surveillance System. Since then, an average of 24 people have died in the state every month from prescription opioid overdoses, and over the last decade, prescription pain medications have been responsible for more drug deaths in Utah than all other drugs combined.
Big pharma to blame?
This rise in prescriptions has hardly occurred in a vacuum. There is a powerful industry, earning stratospheric income from these drugs, lobbying to keep prescriptions up. A shocking new report from the Associated Press claims that the makers of opioid painkillers outspent the US gun lobby on lobbying and campaign contributions by 8:1. In a country where the NRA has been labeled the “Baddest Force in Politics” it is terrifying to see an industry that spends 8 times more than the gun lobby!
During the 9 year period from 2006 to 2015, opioid drugmakers including Purdue Pharma, the maker of OxyContin, spent more than $880 million, or roughly $98 million per year, on lobbying and campaign contributions in support of the drugs, employing an average of 1,350 lobbyists in legislative centers. It is clear that Purdue would want to make sure their products are being prescribed when you realize that they made $2.4 billion from opioid sales last year alone.
There are hundreds of millions of dollars being spent on the marketing of opioids and there has been insistent advocacy from the pharmaceutical industry for these medications. Additionally there is still misinformation that these opioids are not as addictive as other drugs. Far less is spent than these quantities on preventive measures and prescription monitoring programs, not to mention treatment for substance abuse disorder or overdose prevention.
So what happens when prescriptions run out?
As overdose deaths have been on the rise, health care providers, hospitals, pharmacists and regulators have sought to stop prescriptions to those abusing them. However, the solution is not as simple as that. As many as 1 in 4 people who receive prescription opioids long term for non-cancer pain in primary care settings struggle with addiction. You can’t just tell long-term users to stop once their prescription runs out, especially without providing them with follow up services to deal with possible withdrawal symptoms or pain management. Without a medical solution to their addiction, they are left with few options but to resort to the black market in search of illegal prescription opioids or more dangerous available substitutes.
Once users become dependent on pain pills and once their medical providers cut them off, the high price of these opioids on the black market leads some to turn to heroin, which is considerably cheaper and more accessible. On the streets, a pill of OxyContin can sell for as much as $80, whereas a dose of heroin can cost $10.This is why four in five new heroin users started out misusing prescription painkillers. Unfortunately heroin is not even the most worrying alternative as we are now facing the rise of more synthetic opioids, such as fentanyl.
Fentanyl and syntheic opioids creating an even bigger problem
Fentanyl– more commonly known as the drug that pop star Price overdosed from in April– is a substance often given to cancer patients and is more than 100 times as strong as morphine and 30 to 50 times more powerful than heroin. Fentanyl and other synthetic opioids aren’t just more powerful than heroin, they are cheaper and easier to produce, made from chemicals instead of poppies. In some cases, U.S. dealers or addicts are ordering fentanyl or chemically similar drugs online, directly from suppliers in China, which the DEA says produces much of the world’s synthetic opioid supply. Chinese suppliers are also sending large quantities of fentanyl or its chemical ingredients to Mexico, where cartels mix the drug into the heroin supply and smuggle it to U.S. cities. Often, it is passed off as heroin or some other pill and users have no idea that they are taking the dangerous drug. Dealers are also cutting heroin and other drugs with it, because illicit fentanyl is cheap and allows them to stretch their supply.
The presence of fentanyl in street drugs is adding to the growing rise in overdoses. According to numbers from the CDC, from 2013 to 2014, 426% more products tested positive for fentanyl. During this same time period, deaths from synthetic opioids increased by 79%. In 2015, numbers of drug seizures testing positive for fentanyl doubled that 2014 number. Last month, CDC warned about the growing risk of overdose and death from a “widening array of toxic fentanyl-related compounds being mixed with heroin or sold as heroin,” often without buyers’ knowledge. In one example, it pointed to a recent wave of overdose deaths in Ohio tied to carfentanil, an elephant tranquilizer.
Physicians need to lead the change
In late August, Dr. Murthy sent a letter asking doctors for help solving the opioid epidemic. This is the first time in history that the surgeon general has reached out to all physicians, demonstrating the gravity of the situation. In his words “Nearly two decades ago, we were encouraged to be more aggressive about treating pain, often without enough training and support to do so safely. This coincided with heavy marketing of opioids to doctors. Many of us were even taught – incorrectly – that opioids are not addictive when prescribed for legitimate pain.” The letter instructs physicians that they should try other pain relief approaches, such as physical therapy or nonaddictive medications, with most patients before prescribing opioids. If they do choose to prescribe opioids, he instructs them to “start low and go slow” — meaning to prescribe the lowest dose for the shortest duration of time.
This is the first step needed to address the opioid epidemic from its core. Overprescribing has caused a snowball effect, leading to more people using these substances for longer periods of time and resulting in a large number of people with substance abuse and dependence. This abuse has in turn sent many into the black market, where they are trading their prescription pills for more dangerous substances. Combined, it is leading to the highest levels of overdoses and deaths in history. To stop this, we need to not only decrease the number of people entering this vicious cycle with preventive services but we need to make sure we invest in services that will allow us to treat those that unfortunately are already there.


